


 Sign Out
Sign Out

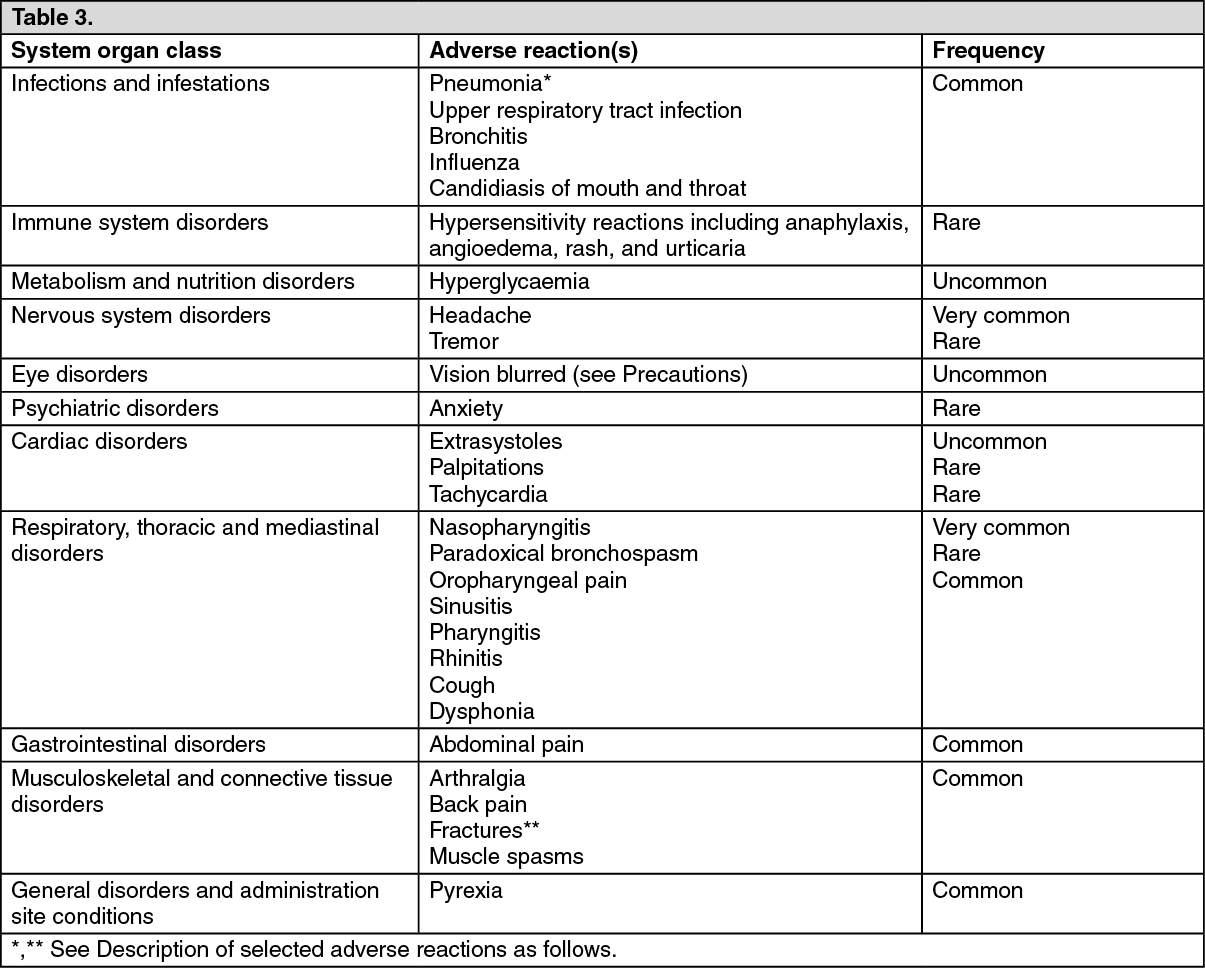
The most commonly reported adverse reactions with fluticasone furoate and vilanterol were headache and nasopharyngitis. With the exception of pneumonia and fractures, the safety profile was similar in patients with asthma and COPD. During clinical studies, pneumonia and fractures were more frequently commonly observed in patients with COPD.
Tabulated list of adverse reactions: Adverse reactions are listed by system organ class and frequency. The following convention has been used for the classification of frequencies: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: *Pneumonia (see Precautions): In an integrated analysis of the two replicate one year studies in moderate to severe COPD (mean predicted post-bronchodilator screening FEV1 of 45%, standard deviation (SD) 13%) with an exacerbation in the preceding year (n = 3255), the number of pneumonia events per 1000 patient years was 97.9 with FF/VI 200/25, 85.7 in the FF/VI 100/25 and 42.3 in the VI 25 group. For severe pneumonia the corresponding number of events per 1000 patient years were 33.6, 35.5, and 7.6 respectively, while for serious pneumonia the corresponding events per 1000 patient years were 35.1 for FF/VI 200/25, 42.9 with FF/VI 100/25, 12.1 with VI 25. Finally, the exposure-adjusted cases of fatal pneumonia were 8.8 for FF/VI 200/25 versus 1.5 for FF/VI 100/25 and 0 for VI 25.
In a placebo-controlled study (SUMMIT) in subjects with moderate COPD (mean percent post-bronchodilator screening FEV1 of 60%, SD 6%), and a history of, or an increased risk of cardiovascular disease, the incidence of pneumonia with FF/VI, FF, VI and placebo was: adverse events (6%, 5%, 4%, 5%); serious adverse events (3%, 4%, 3%, 3%); adjudicated on treatment deaths due to pneumonia (0.3%, 0.2%, 0.1%, 0.2%); the exposure adjusted rates (per 1000 treatment years) were: adverse events (39.5, 42.4, 27.7, 38.4); serious adverse events (22.4, 25.1, 16.4, 22.2); adjudicated on-treatment deaths due to pneumonia (1.8, 1.5, 0.9, 1.4) respectively.
In an integrated analysis of 11 studies in asthma (7,034 patients), the incidence of pneumonia per 1000 patient years was 18.4 for FF/VI 200/25 versus 9.6 for FF/VI 100/25 and 8.0 in the placebo group.
**Fractures: In two replicate 12 month studies in a total of 3,255 patients with COPD the incidence of bone fractures overall was low in all treatment groups, with a higher incidence in all Relvar Ellipta groups (2%) compared with the vilanterol 25 micrograms group (<1%). Although there were more fractures in the Relvar Ellipta groups compared with the vilanterol 25 micrograms group, fractures typically associated with corticosteroid use (e.g., spinal compression/thoracolumbar vertebral fractures, hip and acetabular fractures) occurred in <1% of the Relvar Ellipta and vilanterol treatment arms.
For the SUMMIT study, the incidence of all events of fracture with FF/VI, FF, VI and placebo were 2% in each arm; fractures commonly associated with ICS use were less than 1 % in each arm. The exposure-adjusted rates (per 1000 treatment years) for all fracture events were 13.6, 12.8, 13.2, 11.5 respectively; fractures commonly associated with ICS use were 3.4, 3.9, 2.4, 2.1 respectively.
In an integrated analysis of 11 studies in asthma (7,034 patients), the incidence of fractures was <1%, and usually associated with trauma.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product.
View ADR Monitoring Form